Quantification of coronary artery disease (CAD) burden and atherosclerotic plaque type has been shown to be the strongest determinant of future risk of major adverse cardiac events (MACE).1 Until recently, though, there had been no clinically useful thresholds to help physicians understand a patient’s plaque burden in its entirety to guide CAD diagnosis and management.
Instead, treatment decisions have been all too often based on indirect markers of atherosclerosis. This can result in poor outcomes – 70% of patients who suffer a heart attack had been considered low risk due to the absence of secondary symptoms,2 while nearly two-thirds of referrals for invasive evaluations of the heart based on the presence of secondary symptoms are in fact unnecessary.3
How Atherosclerosis Treatment Algorithms are changing CAD detection
In a recent expert consensus paper in The American Journal of Medicine,4 the Innovations in Prevention Working Group of the American College of Cardiology has introduced the Atherosclerosis Treatment Algorithms. These algorithms provide personalized recommendations for medical interventions based on the combination of coronary computed tomography angiography (CCTA) quantification of atherosclerotic plaque burden and traditional cardiovascular risk factors from existing clinical guidelines.
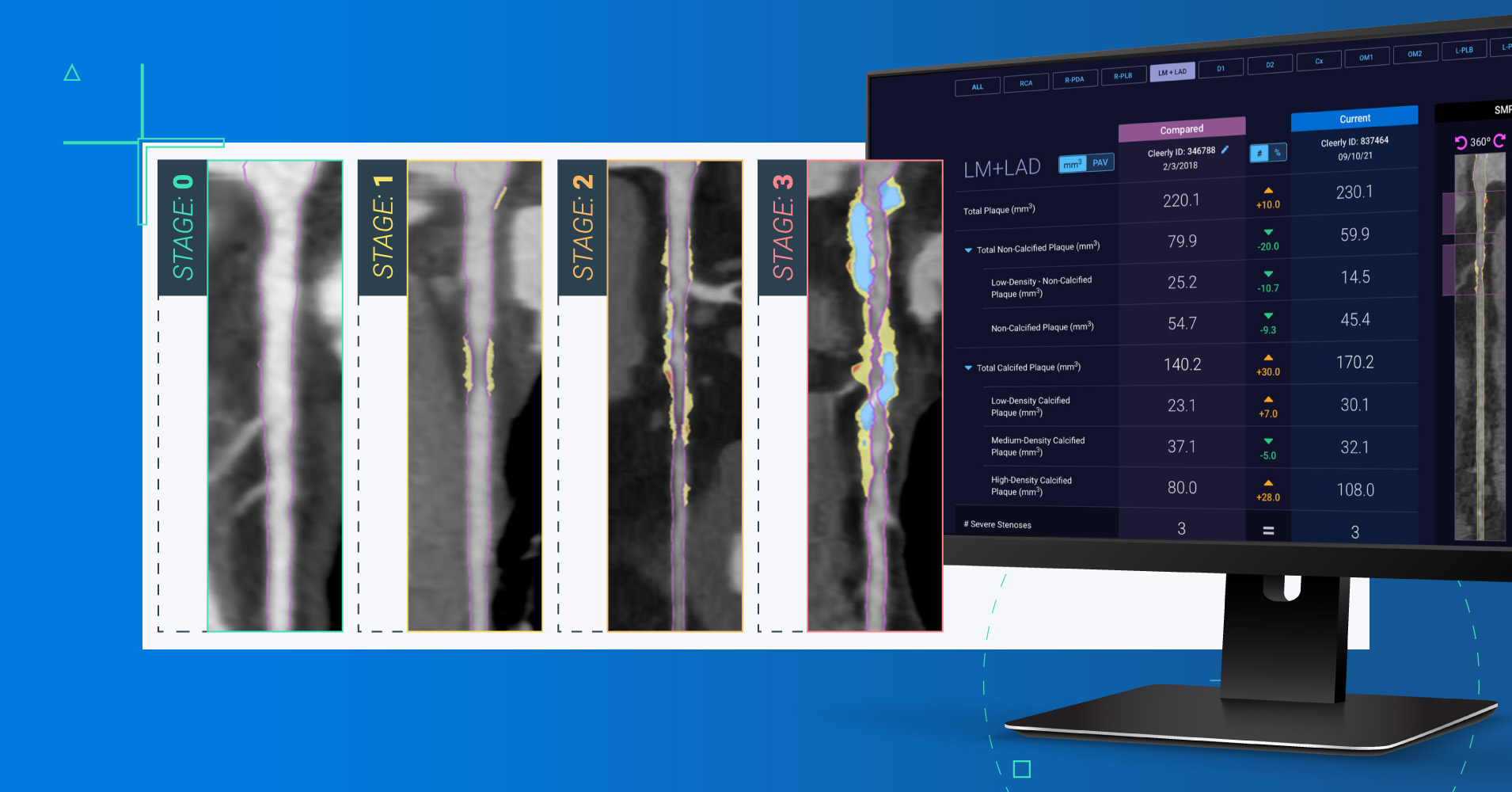
The Atherosclerosis Treatment Algorithms use an atherosclerosis staging system for classifying disease by disease burden, published for the first time earlier this year. To the best of our knowledge, it is the first treatment pathway for heart attack prevention that directly links plaque severity and progression to personalized recommendations for therapy selection and therapy changes, respectively.
Table 1. Stages of Coronary Atherosclerosis by Total Plaque Volume and Percent Atheroma Volume.
Stage of Atherosclerosis
Angiographic Stenosis Severity
Total Plaque Volume (mm3 )
Percent Atheroma Volume (%)
Stage 0
No stenosis
0
0%
Stage 1
1-49% stenosis 1-Vessel CAD >50% stenosis
>0 to 250
>0%-5.0%
Stage 2
2-Vessel CAD >50% stenosis
250-750
>5.0%-15%
Stage 3
3-Vessel CAD >50% stenosis
>750
>15.0%
Algorithms can be used by providers to personalize treatment
CCTA is a non-invasive, highly-accurate method5 of measuring atherosclerotic burden with a low radiation dose.6 It enables a whole-heart quantification of plaque as opposed to a proximal view of single arteries. In addition, when scans are performed at regular intervals, CCTA can be used to assess changes to plaque composition over time.
Much like the atherosclerosis staging system, the treatment algorithms are based on similar prevention models for other common conditions, primarily cancer. In these instances, non-invasive imaging has made it possible to visualize, stage, and classify a disease. With this information, physicians have information that makes it possible to personalize treatment plans based on individual disease characteristics, assess the effectiveness of a given therapy, and change treatment plans over time.
What’s more, the treatment algorithms have been written specifically to account for comorbidities above and beyond atherosclerosis. For example, a patient with Stage 2 atherosclerosis (moderate plaque) and a diagnosis of Type 2 diabetes may receive the recommendation to be prescribed a GLP-1 receptor agonists in addition to a high intensity statin. Meanwhile, a Stage 1 patient (mild plaque) with a diagnosis of dyslipidemia may receive a recommendation to take a statin to manage their cholesterol.
In other words, the Atherosclerosis Treatment Algorithms are positioned to support personalized care pathways for patients based on their individual disease burden, comorbidities, and clinical risk factors. This approach is poised to shift cardiovascular care from a model of reactive response to one of preventive care – and to help providers personalize treatment for millions of Americans every year.
Table 2. Simplified Approach to Medical Therapy Based Upon Stage of Atherosclerosis
Stage
Treatment
Serial CCTA*
Stage 0
Guideline-directed medical therapy / Shared decision for de-escalation of therapy
Cardiac rehabilitation or other supervised exercise program (if covered)
If diabetic, GLP1 receptor agonist and SGLT2 inhibitor
1 year
*Perform serial coronary CT angiographies (CCTA) until plaque stabilization or plaque regression has been achieved.
Next steps for algorithms adoption and refinement
It’s important to note that the treatment algorithms are not intended to serve as a replacement to practice guidelines or consensus statements, nor are they expected to be divorced from risk factor scoring. In addition, treatment algorithms must be validated through randomized trials and observational cohort studies.
That said, the authors of the paper – Cleerly CEO James Min, MD and CMO James Earls, MD, along with representatives from eight leading U.S. medical schools – indicated that the algorithms are expected to evolve to include features such as atherosclerotic plaque composition and diffuseness as well as the presence of high risk plaques.
"We anticipate that there will be a flurry of clinical research in this new field of therapy based upon personalized phenotypic coronary artery disease expression, rather than sole reliance on traditional risk factors. This is the future of cardiovascular care," Earls said.
Disclaimer: The information provided herein is for informational purposes only and does not constitute a recommendation, representation, warranty, statement, or guarantee of any kind. The atherosclerosis treatment algorithms (ATA) are not intended to serve as a replacement to practice guidelines or consensus statements, nor are they expected to be divorced from risk factor scoring. The ATAs are based on the combination of CCTA screenings and traditional cardiovascular risk factors from existing clinical guidelines and are planned to be validated through randomized trials and observational cohort studies.
Sure, the taste of food is important, but do you know how your diet impacts your heart? Many foods contain hidden ingredients that negatively impact...
 Cleerly
Cleerly